Owning and managing a practice is no easy feat, let alone managing multiple practices. Without the proper tools and technologies gathering and analysing data to gain insight into how your practice group is performing is tedious work.
Best Practice gold partner, Cubiko, is excited to announce their new product Cubiko Multisite. Aggregated reporting for multisite practices.
Cubiko is a Practice Intelligence Platform, bringing together over 500 data points for your practice in easy-to-understand dashboards for business insight, increased billings and less stress in managing the practice.
The intelligent business reporting within Cubiko Multisite identifies your top-performing practices and helps you discover areas for improvement. It allows you to gain an understanding of your practice group’s billings and where they are coming from. Additionally, it allows you to identify opportunities to increase revenue and efficiencies across your practice group.
Speaking on the announcement of Cubiko Multisite, Co-founder and CEO Chris Smeed, said, “Cubiko Multisite is an exciting opportunity for the industry to have aggregated data across multiple practices. Cubiko helps you achieve oversight across multiple practices. With over 30 years of combined experience in practice management, the Cubiko team understand how difficult it can be to gain insight into what’s happening in your practice. We’ve created Cubiko, to make practice life easier for you.”
Anyone using Bp Premier, Version Jade and above can click through to the Cubiko website directly from Bp Premier, by clicking on the Cubiko Icon located in the top bar.
Book a demo to learn more about Cubiko Multisite or sign up for their free product, Cubiko Assist.
This article was written and contributed by our partner, Cubiko. Click here to visit their profile on the Best Practice Software Partner Network.
In comparison with other countries, Australia’s COVID-19 vaccine rollout plan was very measured, and the implementation has been somewhat leisurely. With the frequent changes to the guidelines paired with vaccine hesitancy, vaccination hubs and GP clinics around the country have faced many challenges in their quest to immunise the nation.
In theory the government’s plan was considered and robust – vaccinations would be done in phases, where the most vulnerable would be immunized first, and the young and healthy would be immunized last. Millions of doses of the Astra-Zeneca vaccine were ordered, and could be manufactured locally, while fewer of the more expensive Pfizer vaccine was ordered for the most vulnerable.
A central online system was developed that allowed citizens and residents to determine which phase of the rollout they qualified for. Those who qualified for the first phase, aptly titled 1a, would be vaccinated soonest with the Pfizer vaccine at government run vaccine hubs. Those who were 1b or lower in the schedule could book into a participating GP clinic near them to get the Astra-Zeneca vaccine.
Anyone who was involved with the logistics, patient booking, ordering and administration of COVID-19 vaccines was required to complete a five hour online module developed by the federal government to ensure adequate and uniform training of all personnel involved in the vaccine rollout. This included couriers, receptionists, nurses, doctors, and Practice managers at GP clinics around the country.
The plan also involves recording the vaccination details in a centralized system, the Australian Immunisation Register. A lot of groundwork had to be done by software vendors to enable the seamless uploading of this data. This data would help to accurately determine how many people have been vaccinated, in addition to enabling the safety of vaccine administration to ensure they are administered within appropriate time frames. Reactions to vaccines are also being collected to track trends and monitor for any emerging serious reactions.
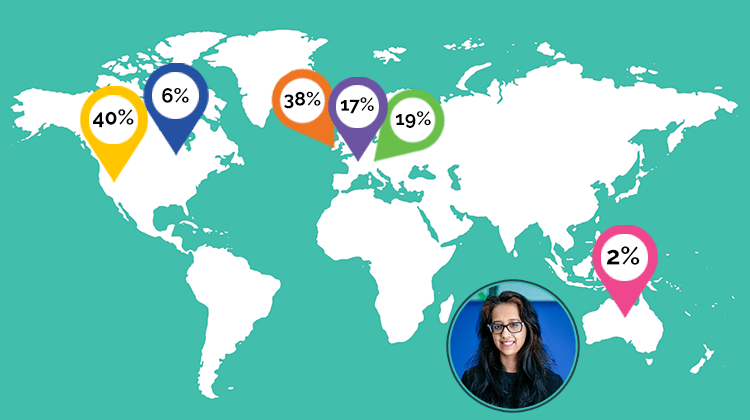
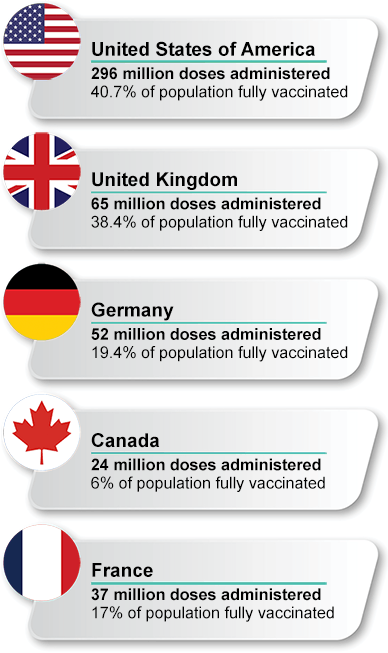
Despite Australia’s COVID-19 vaccine rollout plan, four months into the rollout, as of the 3rd of June only 4.6 million vaccine doses have been administered in Australia, with only 2.1% of our population being fully vaccinated against COVID-19. A rough comparison with other countries with a similar GDP per capita and healthcare systems, over a period of five months paints a startling picture:
The large vaccination numbers in the above-mentioned countries are mostly likely a reflection of the disastrous effect COVID-19 has had socially and economically in those nations, resulting in a more urgent rollout and vaccine acceptance within the community. Given the low level of infections and community transmission in Australia, the immediate benefit of the vaccine is not overtly obvious to many Australians and so the uptake has been slow.
Now with yet another outbreak in Melbourne, a sense of urgency has re-emerged as the public realise the pandemic is still very much a risk to us and this could happen anywhere in the country. Despite the risks of the vaccine, it is clear now from data overseas that the benefit is still greatly outweighed. One of the most common concerns held by those who are vaccine hesitant is the risk of blood clot from the Astra-Zeneca vaccine. Recent Australian data shows 31 confirmed cases of thrombosis with thrombocytopenia syndrome and 10 probably cases, out of a total of 3.29 million doses administered. At the time of writing, the death rate remains at one. Conversely, for every million people diagnosed with COVID-19, 165,000 of those cases (16.5%) experience blood clots as a symptom of the virus.
On the 1st of June 2021, the UK saw its first day without a COVID-19 death. This is a remarkable feat made possible due to their extraordinary vaccination rollout. Similarly, the USA has also seen a significant reduction in mortality and morbidity. Meanwhile other countries, such as Japan, that initially had a slow rollout and low vaccine uptake, are ramping up their vaccination efforts after recent Covid-19 outbreaks.
As a GP who is involved in vaccination counselling and administering the Astra-Zeneca vaccine, the experience has been interesting. From discussing patient concerns, to ensuring informed consent, appropriate documentation, and counselling on the potential side effects in a very short consult has been challenging. There is an immense amount of paperwork and logistical work that is done by my Practice manager and nursing staff to smoothly run the COVID vaccine clinics. Patients are confirmed multiple times to ensure they attend their appointment to avoid wastage of vaccines.
From a funding perspective, our clinic is not making money with this enterprise, but rather we are doing it as a service to the community. For patients, it is much more convenient to have the vaccine at their local and familiar health care centre rather than a large vaccination hub with thousands of other people like we have seen overseas. In some of these centres, both local police and the military have been involved with administering vaccinations.
As medical practitioners we are taught to look at the evidence and what can be deduced from large amounts of data. There is a limited role of anecdata in medicine, yet I still do get asked “What did you do doc? What has been your experience? Is your family ok?”.
I had registered myself to get the Astra-Zeneca vaccine. Despite being considerably concerned about the risk of thrombosis with thrombocytopenic syndrome, I felt the risk of the sequalae of COVID-19 was much worse. After all, what is the point of worrying about the long-term effects of vaccine related complications if I didn’t make it through the pandemic itself? I ended up having to cancel my Astra-Zeneca vaccination as the guidelines changed, and I have subsequently received two doses of the Pfizer vaccine. Overseas, I have elderly relations who have had the Astra-Zeneca vaccine and have either, at worst, had a very mild infection or, at best, had escaped infection all together.
To get through this pandemic, no doubt we all must work together as no one is safe, until everyone is safe.
Authored by:
Dr. Fabrina Hossain Clinical Advisor at Best Practice Software
This product release activity contains important information about enhanced My Health Record functionality that is included in the TOPAZ release of Bp VIP.net.
It is designed to familiarise you with the type of information you can view in My Health Record for your patients, security you can implement in your clinic around accessing My Health Record and uploading both a prescription episode and specialist letters to your patients’ records.
This Be In The Know webinar will cover the Charges Screen in Bp VIP.net.
The webinar will cover the following topics: (Drag the progress bar in the video below to jump to a specific section)
– Navigating around the Charges screen [00:52] – The Provider charge screens [04:29] – Billing per provider [06:39] – The function buttons at the bottom of the screen [08:09] – Setting up Item Fees for private items [10:24] – Looking at the set up of MBS items and copying MBS items [15:09] – Billing Protocols [19:44] – Working with Feescalers [21:28] – Working with Subsidisers [25:39] – Updating fees [26:55] – Assistance Fees – Australia Only [29:18] – Scaling – Australia Only [31:22]
Watch the video and join our expert trainer, Jo Monson, to learn about the Charges Screen in Bp VIP.net!
As you may be aware, ACC is upgrading the current technology used by Practice management software to connect to critical ACC Digital services such as eLodgement and eSchedule.
You may have already started receiving information about this change from ACC, stating that the current methods for accessing ACC Digital services will no longer be available later in the year.
The good news is that Best Practice Software is already working on making the programmatic changes to our software to conform with the new connection requirements, and these will be made available to you later this calendar year.
What does this mean for your Practice?
To ensure that your Practice is not impacted by the ACC connection changes, you will need to upgrade your software when we make it available to you later this year.
From a software workflow perspective, we expect minimal change, and for the transition to using eLodgement and eSchedule API equivalent, to be non-disruptive. We will be providing you with training and enablement material to equip you.
What can you do now to prepare?
If you are using the latest version of Bp VIP.net, Version Ruby SP3 (525.018), no action is required at this time.
If you are on a lower version, we strongly recommend you commence planning now to upgrade to the latest version of the software. This will lessen the impact to your Practice operations when you upgrade to the ACC version of the software later in the year.
We also recommend you notify your staff of the impending ACC software change, in particular, your IT provider.
As soon as we have more information, and our Training team has published enablement resources related to the ACC software update, we’ll notify you through another formal email communication.
Questions? Contact our Support team by phone at 0800 40 1111 or by email at support@bpsoftware.net.
Are you interested in becoming an early adopter of our ACC Digital Services API Integration or do you have further questions?
Contact our team onsupport@bpsoftware.netand we will register your interest and provide further information as we progress our development.
Authored by:
Michael Toulsen Product Manager at Best Practice Software
This Be In The Know webinar focused on Contact Notes will demonstrate how Contact Notes can be utilised in your Practice to provide a high-level of patient care and meet your medico-legal obligations in Bp Premier.
The webinar will cover the following topics: (Drag the progress bar in the video below to jump to a specific section) – What are Contact Notes? [04:07] – Why use Contact Notes and Where can they be raised? [09:24] – Following-up Contacts and Resending Messages [22:00] – Using Contact Notes for Recalls & Reminders [36:49]
Watch the video and join our expert trainer, Bec Bland, to learn about Contact Notes in Bp Premier!
An Update on Medicare Web services – for our Australian Customers
As you may be aware, Services Australia is upgrading the current technology used by practice management software, to connect to critical digital health services such as Medicare/DVA Claiming, Eclipse and the Australian Immunisation Register.
A number of our products currently connect to Services Australia via a Medicare Client Adaptor, which utilises a Medicare PKI certificate also known as a site certificate. As per the new requirements, practice management software vendors will be replacing this Medicare PKI certificate method with a Provider Digital Access (PRODA) account, which will lead to the replacement of the current Medicare Client Adaptor technology.
What does this mean for your Practice?
Practices may have already started receiving information about this change from Services Australia stating that from the 13th of March 2022, the current methods for accessing Medicare/DVA Claiming, Eclipse and the Australian Immunisation Register will no longer be available. To ensure your Practice is not impacted by this change it is extremely important you upgrade to a version of your software that supports Medicare Web services. We expect these updates to be available for our Bp Premierand Bp VIP.net Practices in calendar year Q4 2021 in order to provide our customers with enough time to complete the upgrade prior to the March 2022 deadline.
From a software workflow perspective, we expect minimal change and the transition to using Medicare Web services for Practice staff will be seamless. However, there will be some configuration needed for some products, as part of the upgrade process, to ensure that you have linked your PRODA account as per the new requirements.
Our Training team is busily preparing education sessions, resources and Knowledge Base updates to assist our Practices in preparing and implementing these important changes!
As our Bp Allied product currently uses a third-party solution to deliver Services Australia functionality, these changes will occur in the background. From a software workflow perspective we expect minimal change, and the transition to using Medicare Web services for Practice staff should be seamless. However, there may be some configuration changes in Bp Allied as part of the upgrade process. There is no need for Bp Allied practices to complete any preparation activities at this stage.
What can you do now to prepare? (For Bp Premier and Bp VIP.net Practices only)
If your Practice does not currently have a PRODA account, we suggest creating one ahead of time to ensure you are familiar with its interface and the appropriate authorisation levels are set up for your organisation. This will become important when linking your practice management software (Bp Premier, Bp VIP.net) to your organisation’s PRODA account. If you already have a PRODA account, you can jump right into linking Medicare Online as a service provider to your organisation. Easy to follow steps are provided on the Services Australia website under “Learn how to add and link Medicare Online (including ECLIPSE, DVA and AIR) to your organisation in PRODA.”
We also highly recommend signing up to our training events, downloading our resources and thoroughly reviewing our Knowledge Base once notified that these are available. We expect to have more information regarding these resources at the end of May.
We are currently enhancing our Bp Premier and Bp VIP.net products to support the transition to PRODA and Medicare Web services. This functionality will be made available via our Program Updates from Q4 2021, providing our Practices with plenty of time to upgrade their software and become familiar with web services before the software vendors cut-off date in March 2022.
As mentioned above, our Bp Allied product product currently uses a third-party solution to deliver Services Australia functionality and these changes will occur in the background. From a software workflow perspective, we expect minimal change and the transition to using Medicare Web services for Practice staff will be seamless. However, there may be some configuration changes in Bp Allied as part of the upgrade process.
Are you interested in becoming an early adopter of Medicare Web services or do you have further questions?
Contact our team on MedicareWebservices@bpsoftware.net. We will register your interest and provide further information as we progress our development.
Authored by:
Jessica White Manager of Commercial & Customer Enablement at Best Practice Software
Healthcare consumerism is a concept that has existed for some time, but only recently has it really taken hold and started to significantly impact primary care.
There is perhaps no common understanding as to what constitutes healthcare consumerism, and discussions with providers and patients will likely yield two different sets of responses as to what it actually means.
Ask any provider that has had to contend with correcting the misconceptions of a patient’s self-diagnosis and treatment plan (often courtesy of Dr Google, WebMD or the Mayo Clinic) within the constraints of a few-minutes long consult, and you may be confronted by a somewhat less than flattering take on the subject.
However, as a patient, notions of patient empowerment through clinics and a shift towards patient centricity will likely feature very favourably.
Regardless of your individual view on this, in a consumer-centric society, consumerism was always going to find its way into the healthcare sector, and this will influence the sector in many predictable, but also some unexpected ways. The rate of this change has been accelerating as a result of the general societal changes brought about by COVID-19.
Broadly, consumerism itself has many defining features, but fundamental to it is the principle that the consumer is in control (though subject to marketing, social engineering influences and manipulation). They are in control of what they consume, and their patterns of consumption drive the choices that providers of products and services make about what gets produced and how it is produced. In theory, the more informed consumers are, the more their decisions are driven by knowledge.
It is, then, reasonable to conclude that patterns of consumer behaviour and expectations are responsible for the kind of product and service innovations that organisations like Amazon, Uber and Apple have brought about in their respective industries.
Given the level of disruption that has been brought about by the aformentioned powerhouses in their respective industries, one can only speculate about how much of an impact they would have if they turned their attention to serving the needs of the patient in an era of healthcare consumerism. Even if they don’t – they, and others like them have reset long-held, more traditional consumer expectations.
To compete in this environment, and to compete with the concept of healthcare consumerism itself, provider organisations will have to re-assess their entire value streams, and re-image how to leverage their people, processes and technologies in response to this consumer-centric landscape.
To develop an approach and response, one has to consider some of the behavioural changes brought about by this trend. It does, in essence, come down to the fact that patients’ expectations of care delivery have changed, and that they are taking an increasingly active role through a range of actions.
Patients are, of course, not a homogenous group, so their expectations and their responses to this will differ from one group to another. According to the Pew Research Centre, millennials now make up a larger portion of the population than baby boomers, and the long-term transformations of healthcare will be driven primarily by their needs. This generation has grown up in a technology-rich, consumer focused environment where transparency, rapid delivery and convenience is the norm.
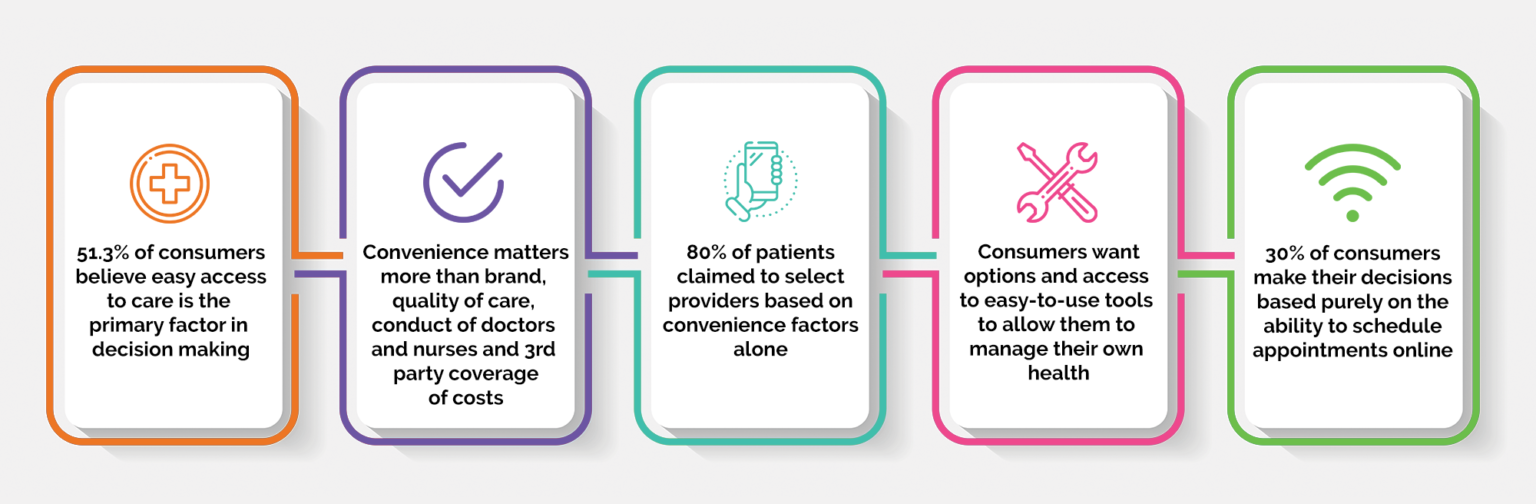
A recent study into healthcare consumer expectations resulted in some startling findings:
As evidenced by the rise in social media, consumers have proven to be willing to share increasing levels of personal information for the sake of convenience across platforms – as a trend in consumer behaviour, this will likely apply in the context of healthcare as well.
It would be reasonable to expect that patients will want to share information between providers (evidencing a willingness to share), will want to have tools to aid this sharing of information (evidencing the importance placed on convenience), but will in all likelihood require more sophisticated consent and sharing models than what is the norm with some non-health related personal data.
Some of the other actions that patients are taking to meet their expectations include:
Shopping around, evaluating their options and generally expecting more from providers
Doing their own research about health issues, treatment options and providers
Taking deliberate steps to monitor and improve their health. The proliferation and increasing sophistication of wearable and home monitoring devices bears witness to this
Co-operating with providers to make treatment decisions and more freely sharing information with care providers
Taking cost and quality aspects into consideration in their decision making
Using technology for appointments, telehealth consults, online payments, prescription renewals and a host of other services
If we consider the expectations and consider the actions patients are taking to meet their expectations, a few things immediately become clear:
Patient loyalty will continue to decrease as millennials make up an increasing percentage of healthcare consumers
Providers will face new challenges in attracting and retaining patients, with less loyal patients being more likely to switch providers, and being enabled to do so with the ease provided by technology
This will have ramifications for health outcomes given the impact on continuity of care
So what’s the message in all of this?
The most logical outcome is that due to the rise of healthcare consumerism, it’s in the industry’s best interest to meet the demands of healthcare consumers by designing products and services that meet current and emerging patient needs.
Here at Best Practice Software, we are developing the next generation of healthcare systems that will not only meet the demands of our provider customers, but software that will deliver the tools and meaningful interactions with patients and other stakeholders to address the needs of future healthcare consumers.
Authored by:
Andre Broodryk Product Manager at Best Practice Software
As the second wave of COVID-19 continues, clinicians remain acutely aware that the pandemic is far from over. Telehealth consultations and electronic prescriptions were two important digital health measures that helped clinicians provide life-saving support whilst protecting patients and staff against the risk of infection.
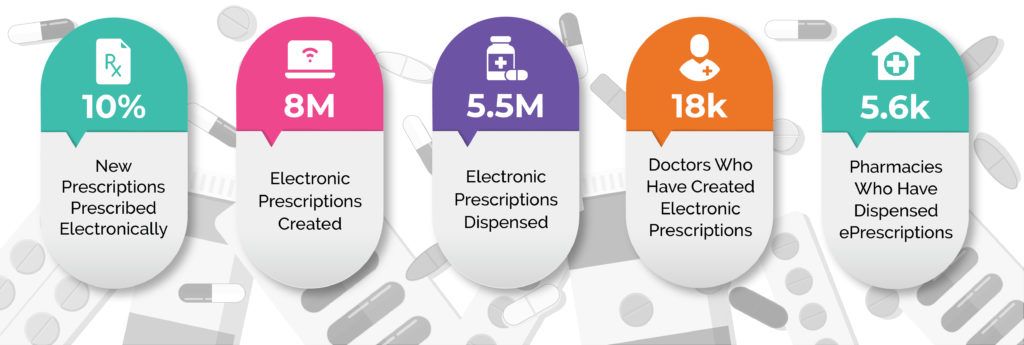
Prior to the introduction of electronic prescriptions in 2019, the patient still needed a paper script. For the past twelve months, as a result of the accelerated national roll out of electronic prescriptions to deal with the pandemic, clinicians have had the option of providing patients with an electronic script via email or SMS rather than a paper script. This provided greater flexibility for patients and reduced the problem of lost or replacement scripts. In the twelve months since, ePrescribing has continued to gain traction, as shown in the following infographic.
Whilst delivering safe, private and efficient prescribing at a distance, Electronic Prescribing has also introduced new clinical benefits. One of the immediate impacts is that clinicians can now cancel an electronic prescription directly from Best Practice Software if the need arises, without having to retrieve the paper script or repeat.
The nation-wide launch of Australia’s first digital script list, called MyScriptList – more accurately referred to as a Department of Health conformant Active Script List (ASL) – also opens up substantial implications for reducing the administrative burden on practices. MyScriptList was launched in partnership by the two national prescription exchange services, eRx Script Exchange and MediSecure. It provides the third national means of access to electronic prescriptions, working alongside the two existing methods of paper scripts and digital tokens (the digitised script sent by a doctor to a patient’s email or phone, introduced in May 2020).
The main clinical benefit arising from the digital script list, or ASL, is that clinicians, patients and pharmacies can now view all of a patient’s current electronic prescriptions and repeats in one digital list. Clinical and administratively, this generates two important changes. Firstly, it removes problems associated with patients losing or not being able to locate the correct script, as their digital script list will always be current in real-time. This reduces the administrative load of re-issuing and re-sending scripts and repeats. Secondly, a combined digital script list makes it significantly easier for clinicians and pharmacies to support patients who have chronic health issues.
The successful rollout of Electronic Prescribing during the pandemic can be largely attributed to the twelve plus years of safe and secure electronic prescription transfer through eRx Script Exchange. eRx functionality, prior to the advent of electronic prescriptions, operated as a parallel electronic process to doctors’ paper-prescribing. eRx helps to ensure prescriptions are dispensed as the prescriber intended, reducing the possibility of misinterpretation or accidental dispensing errors. With more than 31,000 doctors and 5,500 pharmacies using eRx to handle 90% of prescriptions, the system has provided a proven and secure pathway to electronic prescriptions.
In the twelve years since, the prescription exchange service has become the backbone for a range of clinical tools that provide visibility of a patient’s current medication and treatment. Real-time prescription monitoring of Schedule 8 drugs is an example. This displays an alert if a patient’s interactions are at risk of causing an adverse event. According to the Victorian Coroners Court, Victoria’s real-time prescription monitoring, SafeScript, has contributed to reversing a 10-year trend of increasing prescription medicine overdose deaths (showing a reduction for the first time in 10 years, from 405 deaths in 2019 compared to 424 deaths in 2018).
Whilst more attention needs to be given to the follow up mechanisms that support patients once a red flag is identified, real-time interaction flags are a vital clinical tool to help protect patients with dependencies on monitored drugs – and the devastating toll that this takes on their families and communities.
Best Practice Software CEO, Dr Frank Pyefinch, has been an advocate of ePrescribing and sent the very first electronic prescription from our Bp Premier software back in 2009. “Electronic prescribing has come a long way since its early conception back in 2009, which initially focused on the reduction of medication errors from the manual entering of prescription data by pharmacists into their dispensing software. Now clinicians can send prescription data to their patients without the need for paper, making things like telehealth consultations and the good old, ‘I lost my prescription,’ workflows more efficient and safer for both practices and patients.”
“The introduction of other initiatives like real time prescription monitoring (RTPM), under the electronic prescribing umbrella, have introduced additional important clinical safety measures and provided clinicians with important medication data at the point of care. We continue to see great innovation in this space, with plenty more planned changes on the horizon.”
Connecting to a prescription exchange service is fundamental to increasing the visibility of patient medication information, which increases your control over medications. Connecting all of your clinicians to a prescription exchange service is the start.
Co-authored by:
Dr Frank Pyefinch CEO at Best Practice Software & Paul Naismith CEO at Fred IT
Leading clinical software provider Best Practice has announced an enhanced partnership with digital health company, HealthShare, by elevating its partner status to the top-tier Bp Partner Network Gold status, one of only 6 partners across the entire partner network.
The designation of the Gold partner status is in recognition of the seamless integration with Bp Premier and the strong utilisation of HealthShare’s products – Referrals Directory, BetterConsult and FactSheets – by Bp Premier users.
A recent GP survey showed 71% of GPs used HealthShare’s Referrals Directory within Bp Premier. The Directory includes comprehensive and up-to-date information about private practising specialists and allied health providers, helping the GP quickly and easily make their right referral decision for their patient. It also reduces admin burden for practice staff by ensuring they don’t need to maintain their local address book.
BetterConsult helps provide GPs with a concise clinical summary of the patient’s agenda before the consult begins, helping to streamline consults, reduce admin burden for the GP and improve the GP-patient interaction. With universal COVID-19 screening, it also helps support practice staff with managing their at-risk patient cohort.
With FactSheets, GPs can quickly access a comprehensive collection of evidence-based condition and medication information from leading Australian and international organisations, helping to support patient understanding and improving health literacy.
Speaking on the partnership Dr Frank Pyefinch, CEO of Best Practice, said, “HealthShare has been a trusted partner since 2014 and it is very pleasing to see the continued growth in usage of their products through BP Premier. Their continued investment in product innovation aligns well with Best Practice’s mission to support doctors with quality products that help deliver better patient care.”
HealthShare Co-Founder, Rami Weiss, said, “We have had an excellent partnership with Best Practice and look forward to continue working together to build products that can help support their users.”
See what GPs are saying about BetterConsult – click here.
See what GPs are saying about Referrals – click here.
For any media enquiries, please contact:
Andrew Simpson Senior Marketing Manager, HealthShare