Best Practice Software is in the final phases of getting ready to release My Health Record functionality for specialists through Bp VIP.net – a software solution that serves the needs of medical specialists such as ophthalmologists and cardiologists.
During 2019, the Australian Digital Health Agency (ADHA) invited leading software vendors for specialists to co-produce design improvements to their experience with My Health Record (MHR). Bp VIP.net was accepted as a software vendor to participate in joint workshops organised by the ADHA to improve MHR functionality and overall usability for all specialists in Australia.
The end-result of the collaboration is a dedicated Bp VIP.net software release for My Health Record functionality, due for public release in early 2021.
The media release published by the ADHA is available here.
From Understanding Specialist Workflows to Improving User Experience and Patient Discovery
One of the key drivers behind the My Health Record for specialists initiative, and for software vendors to participate in joint workshops, was to increase a joint understanding of specialist needs. The goal of the joint understanding is to improve overall My Health Record functionality with software vendors and to avoid disrupting specialist and Practice workflows by providing a better user experience.
Taking this approach, Best Practice Software wanted to streamline all integration points in Bp VIP.net to My Health Record to ensure ease of access for viewing, accessing and downloading patient records. With the design improvements, we also wanted to ensure the same streamlined approach for uploading clinical documents back to My Health Record. This will ultimately lead to improving the overall shared electronic patient record in Australia and bettering the care of patients.
One of the long-term goals for the ADHA is to continue to increase the overall uptake of My Health Record amongst medical specialists. As the uptake for MHR has been significant over the years through our Best Practice GP software, Bp Premier, we also needed to ensure an integrated design approach for specialists. This ultimately leads to offering a great user experience to all users of Bp VIP.net software. Access to electronic patient records through MHR has been streamlined in all relevant specialist’s features to blend into existing Practice workflows. The release provides access to new MHR functionality while minimising disruption to Practices and increasing ease of access and uploads to MHR.
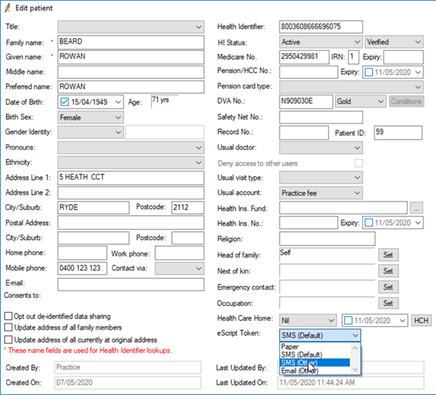
Patient discovery is another crucial aspect for a successful MHR user experience. One of the outcomes of the My Health Record design process, has led to helping specialists identify whether a patient has a MHR and whether they are actively participating in the program. Bp VIP.net users can easily identify patient participation through improved MHR status updates in the software.
When is This Becoming Available for Specialists?
Bp VIP.net is in the final stages of development and are getting ready for general release in the beginning of 2021, to offer specialists an integrated and seamless experience with My Health Record.
Offering a great user experience has been at the heart of the design process, while ensuring a safe and secure approach to managing patient privacy and consent to MHR. Improved healthcare outcomes have already been proven by the uptake of MHR and the improved functionality for specialists will hopefully keep us moving in the right direction with the technology available to all of us today for managing a shared health record.
Authored by:
![]()
Henry Vesander
Product Management Leader at Best Practice Software