
It’s now been approximately 8 weeks since the Australian government mandated that those prescribing medication needed to include the active ingredient names when preparing a prescription.
The introduction of active ingredient prescribing from the 1st of February 2021 presented many doctors with considerable changes to the way they were prescribing medication. The legislation requires prescriptions to include a medication’s active ingredient first, then optionally followed by the brand name. This means that prescriptions can no longer only have the brand name listed, unless they are included in the “List of Excluded Medicinal Items” (LEMI).
A significant amount of groundwork was required for software vendors to implement the changes. Medical Practices across Australia had to upgrade their prescription generating software to ensure they were meeting their legislative obligations.

Prescribing Medication by Active Ingredient - Dr. Fabrina Weighs in 8 Weeks On
Most Practice management software solutions provide easy and seamless processes to prescribe new medication and re-prescribe existing medication. The new legislation now requires doctors to add additional steps to their existing workflow when prescribing medication if they want their patient to have a specific brand dispensed by the pharmacist. As with all systemic changes, major or minor, there were significant challenges faced by doctors with the introduction of this change.
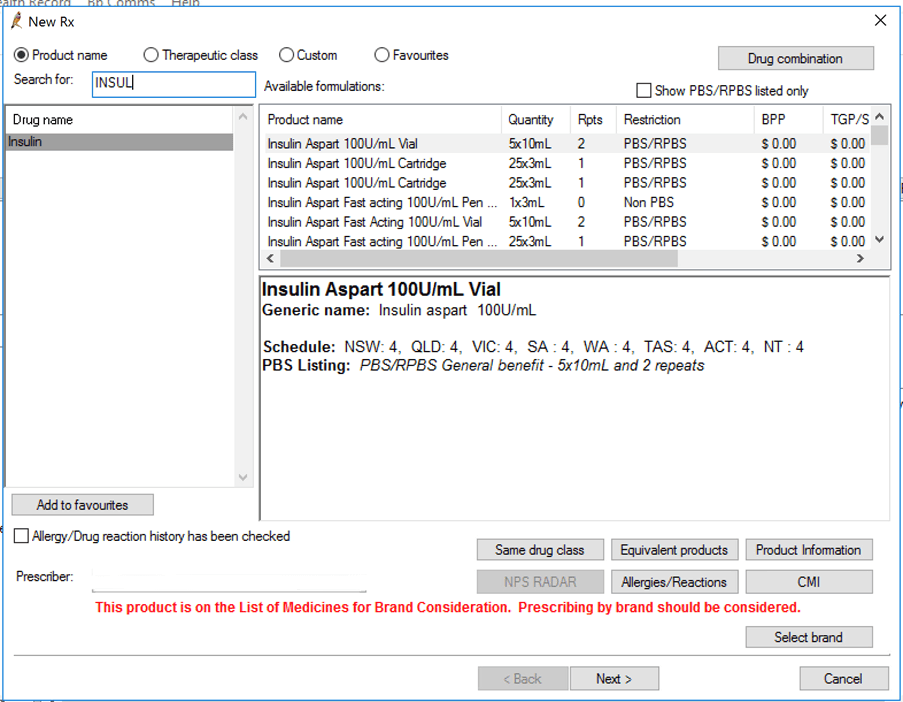
In the early days of the changeover, it was common to omit the additional step to check the “Print Brand Name on Script” field and as a result, prescriptions that should have had the brand name listed only had the active ingredient printed. This posed potential dangers especially for medications such as insulin with a narrow therapeutic window, and for the combined oral contraceptive pill with multiple brands with the same active ingredient that are not necessarily interchangeable. While these medications are not in the aforementioned “List of Excluded Medicinal Items” (and therefore software vendors could not automatically print the brand on the script), they are included in the government’s “List of Medications for Brand Consideration” (LMBC). The LMBC is a list of medications the government has deemed that, due to safety reasons, should be prescribed by brand name.
In Bp Premier, when prescribing medication, there is now a warning message that highlights if a brand name should be considered – this is based on the LMBC list mentioned above:
This change has obligated doctors to have discussions with their patients about their medication, the active ingredient name and if there is a clinical or non-clinical reason why they should be taking a specific brand.
Some common clinical reasons why a brand should be prescribed can include, but are not limited to; medications that are not bioequivalent such as Eltroxin and Eutroxig/Oroxine; different medication formulations such as extended release or immediate release; drugs with different dosing frequency, for example, certain oestrogen patches; allergies or intolerances to other additives such as gluten or lactose; and patient specific idiosyncratic reactions.
Non-clinical reasons why doctors may wish to prescribe by brand name for certain populations such as those with low literacy rates, disabilities or those coming from culturally and linguistically diverse backgrounds who may find it easier to identify their medications by its packaging. If there are no compelling reasons to continue with a specific brand, we should discuss the option to switch to a generic brand thereby facilitating informed decision making by the patient.
Although generic medications have been available in Australia for many years, some patients still have misconceptions regarding perceived poor quality and therefore reduced efficacy and safety of generic medication. It should be stressed that generic medications are not akin to “home brand” items found in supermarkets as these medications have been approved by the TGA and are deemed to be bioequivalent and just as safe and efficacious as their brand-named counterparts by clinical studies. While these discussions naturally add to our consult time, they are important to aide in patients overall understanding of their condition and treatment plan when prescribing medication.
As predicted by the Department of Health, this change will achieve several benefits to both patients and taxpayers. It is envisaged that active ingredient prescribing will increase consumer health literacy and make communication less ambiguous thereby reducing the risk of patients doubling up on medications or omitting to take them by mistake. There will also be a significant reduction in the cost of medications to patients and improvement in the financial sustainability of the PBS and RPBS with the increased uptake of generic medication.
The use of active ingredient prescribing is already implemented in hospitals nationwide and the extension to primary and community-based care was inevitable. While patients, doctors and pharmacies faced some hurdles initially, for the most part these have been overcome with diligence.
For more information, read our article discussing what active ingredient prescribing means for you.
Authored by:
![]()
Dr. Fabrina Hossain
Clinical Advisor at Best Practice Software