Building the Best Health App has certainly been a journey. It’s progressed from an initial idea to countless workshops, engaging with our customers at the 2017 Bp Summit for feedback on desired features and functionality, a bit of external consulting, creating our own internal app team, starting a multiple stage testing process, and live beta sites, all before the public release.
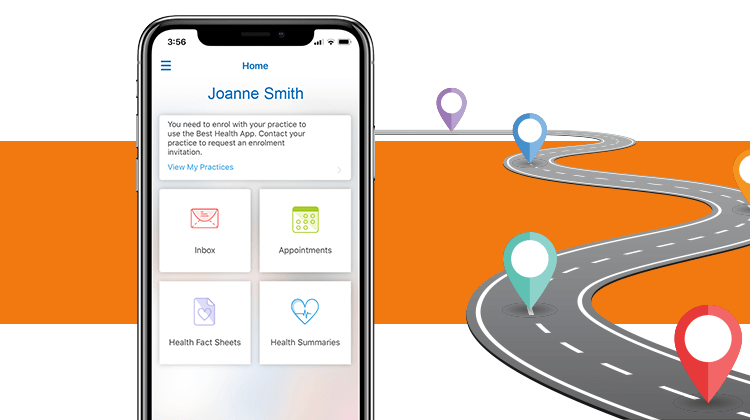
Our journey started with an idea and vision to bring a patient’s health record right into their own pocket empowering them to take control of their health care journey. So, no matter where a person is travelling, they can always access their clinical information to improve the care that they receive.
This idea quickly gained traction as it also provides a completely new way for Practices and Doctors to engage with their patients and improve their overall relationships. It opens the door to the concept of Patient Experience (PX) and the first consumer facing product for Best Practice Software.
We engaged an external agency, experienced in app design, to ensure our technical design followed the latest industry standards, security models and technologies.
We then put together our own internal team which grew to six dedicated developers as well as additional supporting technical staff. The team works across both the Best Health App and Bp Premier Practice Management System ensuring a seamless integration between the two products. Our subject matter experts (SMEs) and the broader team across the business also played a pivotal role in identifying the product requirements for each feature.
Getting to public release required a highly collaborative approach across all areas of our organisation to ensure that we were ready to give practices the best possible customer experience. Training, sales, marketing, support and legal all had to come together for us to make the public release a reality.
Yeah Nah, Not So Simple…
Things are always more complex than they seem initially, and we have faced many challenges along the way that have required significant effort and collaboration by the team to resolve.
Challenges are opportunities and we welcome them.
One of the ongoing challenges is balancing out the integrated feature work between the Best Health App and Bp Premier. This required cross-team coordination to ensure the two products worked seamlessly together. As an example, we created a Patient Check-In feature in the app, which required substantial integration work to ensure we adhered to the patient identification criteria outlined by the RACGP and meets the standards of patient identification in Australia.
The messaging component between the Best Health App and Bp Premier provided many challenges. We started with a straightforward requirement for doctors to be able to send messages to patients that soon morphed into a complex exception management framework with identified points of failure and defined recovery methods. The result being a streamlined experience driven by preferred communication based on patient preferences. The Best Health App includes many types of messages such as appointment and clinical reminders, patient education material and practice notifications. This solution decreases overall messaging costs and creates savings for practices.
Privacy & Security
Security, privacy and storage of patient’s sensitive data is critical and forms the architectural backbone of the Best Health App. The team engaged with security experts to solution a framework that met the security and privacy guidelines necessary for this type of patient app. The outcome is a platform that enforces Australian data sovereignty and ensures we are using the latest encryption methods and tools available. As testimony to all this hard work, we received a very high security score for the penetration testing that was conducted by an external party.
In addition, we completely remodelled the Patient Consent process to help manage Patient Privacy, giving patients the choice of communication types, they wish to receive. The Patient Consent process was part of the Bp Premier Indigo SP1 release and received a significant amount of positive feedback from external parties.
Exciting Times Ahead
It has taken us close to three years to get to this point where we are confident that we have the right architectural framework to ensure all bases are covered in respect to Practice and patient confidentiality and the security of all personal and clinical data. We have a solid foundational product that is clinically and technically safe and effective, upon which we can confidently build more features for Practices and patients to meet the growing need in the community to have greater flexibility and control over their time and access to clinical information.
With an ever growing percentage of people accustomed to doing almost everything online at a time that fits in with a hectic lifestyle, having a trusted app that connects patients to their Practices, where they can manage medical appointments, reminders and other clinical information in the one place can provide peace of mind and empower people to take control of their health care journey.
This is an exciting time for everyone involved and we cannot wait to release more features and continue to enhance patient experience for our industry.